
A breakout on your back. A few extra hairs in the shower drain. A lingering puffiness in your chest. A blood pressure reading that’s crept into the red. In the world of performance enhancement, these are often dismissed as the “price of admission.” But they are far more significant than mere annoyances. They are your body’s biochemical warning lights—visible and measurable signals of internal, systemic stress caused by altering your core endocrinology.
This guide provides practical, evidence-based strategies to manage the four most common and concerning side effects of AAS use. Crucially, it does so with a foundational truth: mitigation is not magic. These effects are direct, dose-dependent consequences of your choices. True management begins not with finding the perfect pill to hide the symptom, but with understanding and respectfully responding to the underlying harm.
The Androgenic Onslaught: Acne and Hair Loss
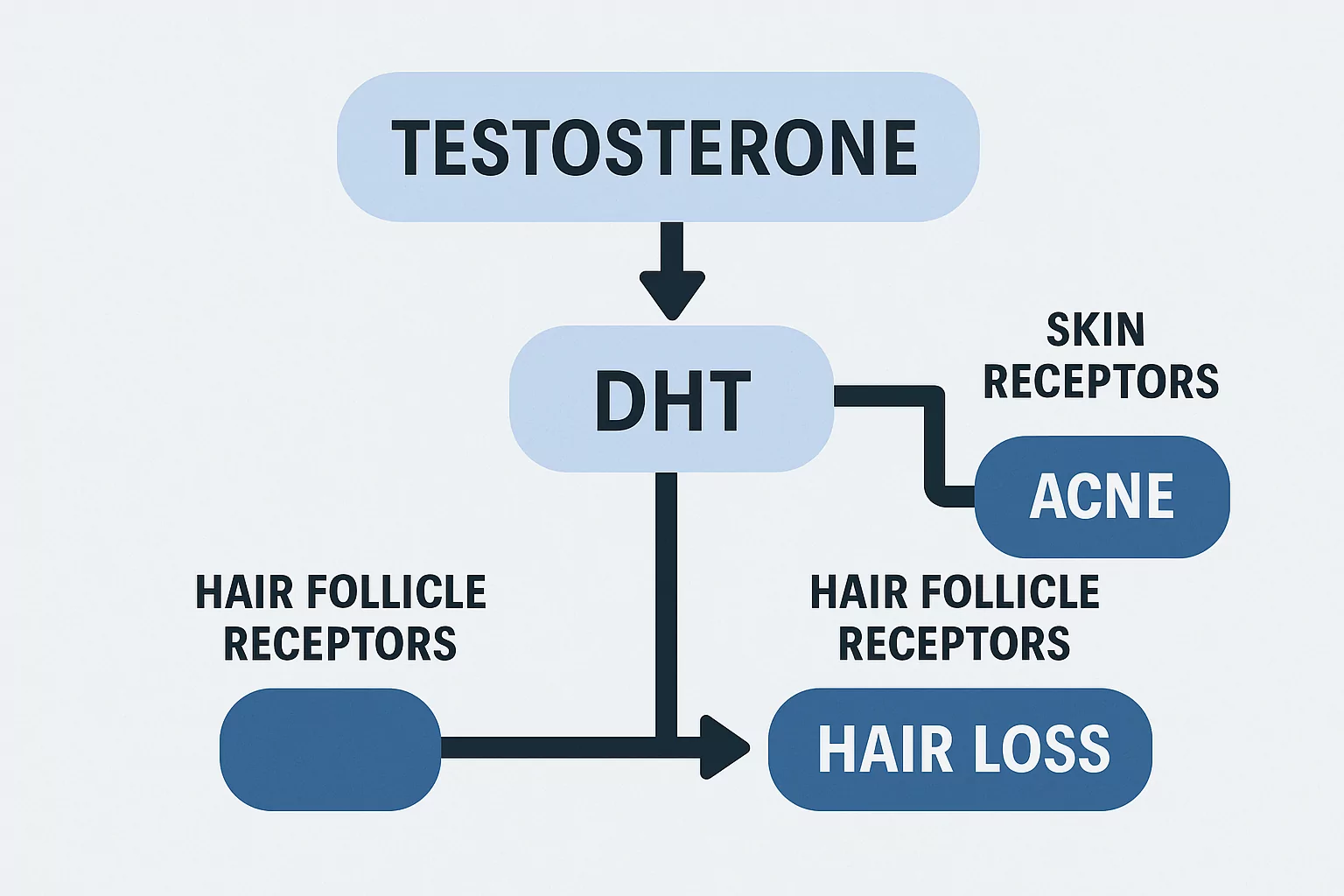
Acne and hair loss share a common driver: androgen receptor activation in sensitive tissues. When you introduce exogenous testosterone, your body often converts a portion of it into Dihydrotestosterone (DHT), a more potent androgen that binds strongly to receptors in the skin and hair follicles. For a deeper look at this fundamental mechanism, see our article on what AAS are.
Acne: More Than Skin Deep
On-cycle acne is typically hormonal and inflammatory. Androgens increase sebum (oil) production and alter its composition, clogging pores and creating an environment where C. acnes bacteria thrive.
The Mitigation Ladder:
- Topical Arsenal: This is your first line of defense.
- Benzoyl Peroxide: An antimicrobial that kills bacteria. Start with a 2.5-5% wash or gel.
- Topical Retinoids (Adapalene, Tretinoin): Gold standard for increasing skin cell turnover and preventing clogged pores. Require consistency and sunscreen.
- Salicylic Acid: A beta-hydroxy acid that exfoliates inside pores.
- Oral Antibiotics (A Short-Term Fix): For moderate inflammatory acne, a doctor may prescribe doxycycline. This is a temporary suppressant, not a cure, and disrupts gut microbiome.
- The Nuclear Option: Accutane (Isotretinoin): For severe, cystic acne, this is the most effective treatment. It is also extremely hepatotoxic and negatively impacts cholesterol. Combining Accutane with oral steroids is a recipe for severe liver strain and must only be done under strict medical supervision with regular blood work.
Hair Loss (Androgenetic Alopecia)
Steroids do not cause baldness in a vacuum; they accelerate it in those genetically predisposed. If you have the genes for male pattern baldness, DHT will miniaturize your hair follicles, shortening the growth phase.
The Mitigation Toolkit:
- Topical Minoxidil: A vasodilator that can extend the growth phase of hair. It works for some, but requires lifelong use and is a maintenance tool, not a cure.
- Oral Finasteride/Dutasteride: These 5-alpha-reductase inhibitors block the conversion of testosterone to DHT. Critical Warning: They can have systemic side effects (e.g., sexual dysfunction, mood changes) and their use with 19-nor compounds like Nandrolone or Trenbolone is controversial and may worsen hair loss through other pathways.
- Ketoconazole Shampoo: Has mild anti-androgenic properties and can be a useful adjunct.
The Harsh Reality: For the highly predisposed individual using potent androgens, pharmacological intervention is often a delaying action. The most effective strategies are choosing less androgenic compounds or accepting the trade-off.
The Estrogen Dilemma: Gynecomastia
“Gyno” is the development of breast gland tissue in males, caused by an imbalance between estrogen and androgens, typically from the aromatization of testosterone into estrogen.
The Prevention and Management Hierarchy:
- Primary Prevention (On-Cycle): The goal is to manage estrogen, not annihilate it.
- Aromatase Inhibitors (AIs): Drugs like Anastrozole reduce the conversion of testosterone to estrogen. They are a preventative tool. Dosage should be guided by estradiol levels from blood work, not guesswork, to avoid crashing estrogen (bad for joints, mood, and lipids).
- Addressing Early Signs: If you feel itchiness, tenderness, or puffiness behind the nipple, it’s time for a SERM.
- Tamoxifen (Nolvadex): Acts as an estrogen blocker at the breast tissue receptor. A common protocol is 10-20mg daily until symptoms subside, often used alongside a slight AI adjustment.
- The Point of No Return: Once firm, fibrous glandular tissue has formed (usually after several months), surgical excision is the only permanent solution. Pharmacological interventions can only shrink or prevent, not remove, established tissue.
The Silent Killer: Hypertension
High blood pressure is the most dangerously underestimated side effect. It causes silent, cumulative damage to your heart, kidneys, and blood vessels. On cycle, it’s typically caused by a combination of factors from our list of common side effects of steroids:
- Increased Hematocrit: Testosterone boosts red blood cell production, thickening your blood and increasing peripheral resistance.
- Water & Sodium Retention: Elevated estrogen and some compounds promote fluid retention.
- Sympathetic Nervous Activation: Androgens can increase aggression and stress responses, constricting blood vessels.
- Endothelial Dysfunction: Some AAS directly impair blood vessel elasticity.
The Management Protocol (Lifestyle First):
- Monitor Religiously: A home blood pressure cuff is non-negotiable. Track readings in the morning and evening.
- Cardio & Hydration: Consistent aerobic exercise (30-45 mins, 4-5x/week) is one of the most effective tools to improve vascular health and lower resting BP. Drink plenty of water.
- Dietary Support: Reduce sodium intake, increase potassium (avocados, leafy greens), and consider supplements like aged garlic extract or magnesium.
- Pharmaceutical Intervention: If lifestyle measures fail and BP remains consistently elevated (e.g., >140/90), medical intervention is required. A doctor may prescribe an ARB like Telmisartan, which is often favored in fitness circles for its potential PPAR-gamma benefits and good side effect profile. This is a prescription medication and requires a doctor.
The Unified Principle: Side Effects as Feedback
The severity of every side effect discussed is intrinsically dose and compound-dependent. They are not random; they are feedback. The most effective “management” tool is often the least popular: dose reduction or choosing a milder compound.
This is the core of the myth of the “safe” cycle. You cannot indefinitely outmaneuver the fundamental pharmacology of powerful hormones. Management strategies—whether topical creams, SERMs, or BP meds—are a holding action. The prudent long-term strategy for minimizing sides is intelligent cycle design: shorter durations, conservative doses, and ample time off.
Conclusion: Responsible Management as Part of the Journey
A successful cycle isn’t defined by the absence of sides, but by your intelligent, measured response to them. Before reaching for a new drug to solve a problem, ask yourself:
- Do I have current blood work to inform my decision?
- Can I adjust my dose or compound?
- Am I using the correct, targeted pharmaceutical for this issue (e.g., a SERM for gyno, not an AI crash)?
Manage with intelligence, but respect the warnings. Your body is communicating the very real, systemic impacts of your choices. The smartest athletes are the ones who listen, adapt, and never forget that they are negotiating with their biology, not commanding it.